

If you want to watch this content on YouTube, click here.
What is LPR?
LPR is known as silent reflux. It’s because classic reflux symptoms like heartburn are often absent.
But it’s a form of reflux where the contents from your stomach including:
- Acid
- Pepsin
- Often bile
- Other intestinal contents
travel up the esophagus to the throat, larynx, sinuses, and eustachian tubes and can even be aspirated into the lungs.
This process can cause a variety of symptoms including:
- Hoarseness
- Sore or burning throat
- A bitter taste
- Throat-clearing or cough
- Difficulty swallowing
- Globus, a feeling of a lump or something stuck in the throat
- Wheezing, breathing difficulty, or asthma-like symptoms
- Postnasal drip
Gas, bloating, belching and heartburn may or may not be present.
While some of these symptoms can be caused by other things like:
- Viral or bacterial infections
- Smoking
- Vocal abuse
- Allergies
- Pollution
- Other irritants
chronic symptoms are often a result of persistent reflux. If you suffer from these symptoms on a regular basis, there is a good chance you have LPR.
Now what to do about LPR
The most recommended treatment is acid-reducing medicines including PPIs and H2 blockers.
But do these really work for LPR?
According to the systematic review titled, Management of laryngopharyngeal reflux with proton pump inhibitors:
“Data from these trials show that PPI therapy is no more effective than placebo in producing symptom relief in patients suspected of LPR.”
The same conclusions were also reached in 2016, Meta-analysis of the efficacy of proton pump inhibitors for the symptoms of laryngopharyngeal reflux:
“The difference between PPIs and placebo groups in the overall improvement of symptoms in adult patients with LPR was not statistically significant.”
As a result, the American Gastroenterological Association guidelines for GERD recommended against the use of acid-suppression therapy for the treatment of patients with extraesophageal GERD syndromes (laryngitis, asthma).
So, what’s wrong with acid-reducing medicines?
Why don’t they work better than the placebos?
The most likely reason is that they only reduce stomach acid and have no effect on:
- Pepsin
- Bile salts
- Bacteria
- Pancreatic enzymes
- Other components of reflux
that are perhaps more damaging than stomach acid for LPR.
PPIs can also work against you because they can promote SIBO according to some studies. And it’s the gas pressure from SIBO that I have proposed as the underlying cause of reflux.
To address LPR, we must control reflux itself.
Why must we control reflux for LPR?
Is there evidence this works?
Yes!
Surgically stopping reflux via a fundoplication operation resulted in a 73 to 83 % improvement in:
- Voice fatigue
- Chronic cough
- Choking episodes
- Sore throat
- A lump in the throat
- Throat clearing
Even asthmatic symptoms improved 60% according to a 2011 study, Impact of Nissen fundoplication on laryngopharyngeal reflux symptoms.
I am not recommending this procedure as first-line therapy due to risks and potential side effects, but this is a proof of the principle that stopping reflux is the key to controlling LPR symptoms instead of blocking acid.
How do we stop reflux for LPR, without drugs and without surgery?
Could food have something to do with it?
There are a couple of diet approaches often recommended for LPR:
- Trigger food diet
- Low acid diet
Both of these are the same as the approach used for GERD.
The use of the trigger food approach is pervasive, but it has been debunked by the American Medical Association’s Continuing Medical Education program. Here is the quote, “routine global elimination of foods that can trigger reflux is not recommended for the treatment of GERD.”
How about Low Acid foods?
The low acid approach focuses on the stomach enzyme called pepsin which helps digest protein. But when it refluxes into the throat and surrounding tissue, its presence becomes inflammatory. Because this enzyme is only active at an acidic pH, the strategy is to avoid acidic foods such as:
- Tomatoes
- Vinegar
- Fermented or otherwise preserved foods
- Many fruits, including citrus
- Certain spices
- Coffee
- Soda, etc.
because these foods might activate it.
While this approach makes rational sense, it does not include an element to control or stop reflux, and rather deals with reflux after the fact. Making the picture a bit more complicated, I mentioned that in addition to pepsin, reflux also contains:
- Acid
- Bile
- Other digestive enzymes
- Bacteria and their end products
The impact of these other elements will not benefit from a low acid diet.
LPR Diet – Is there any dietary approach that is designed to stop reflux?
To answer this question, we need to understand the cause of reflux and how it occurs.
For the last 60+ years, the cause of reflux was believed to be that the lower esophageal sphincter muscles, or LES at the top of the stomach either become weak or relax at the wrong time. I believe this theory is inaccurate or at best incomplete and have proposed a different idea in my books Heartburn Cured and Fast Tract Digestion Heartburn.
There is solid evidence that reflux is caused by poor digestion of carbohydrates, which just so happens to be the favorite fuel for most gut bacteria. When too many carbs are not fully digested and absorbed into your bloodstream, they persist in the intestine and can feed blooms of gas-producing bacteria.
Only 30 grams of unabsorbed carbs can allow gut bacteria to produce over 10 liters of gas in the intestines.
This gas eventually makes its way to the stomach. The idea is that this intragastric gas pressure puts pressure on the LES eventually forcing it open and allowing reflux to occur like Mentos in a coke bottle. This increased intragastric pressure is well documented in people with reflux.
How do we translate this into an action plan for LPR?
Looking through this lens, the sound solution for LPR is to stop reflux by depriving your gas-producing gut bacteria of excess carbohydrates. And you can do this by limiting hard-to-digest fermentable carbohydrates. These include:
- Lactose
- Fructose and polymers of fructose
- Resistant starch
- Fiber
- Sugar alcohols (exception erythritol)
The Fast Tract Diet I developed is designed to accomplish this. The Fast Tract Diet systematically limits the full spectrum of hard-to-digest fermentable carbohydrates in your diet. Based on the food type and serving size, each food or drink is rated by a point system I created called FP, fermentation potential.
The lower the points for each food and drink, the lower the symptom potential.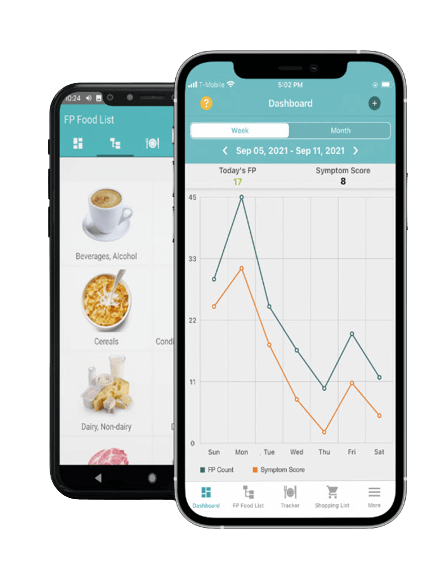
The Fast Tract Diet mobile app makes it easy to implement the diet. It lists over 1,100 foods based on their FP points, and there is a built-in calculator to determine the points of other foods as well.
You can track your meals, FP points, and symptoms in the app so that it will automatically chart the relationship between your points and symptoms.
You can read the Fast Tract Diet mini-chapters in the app before starting the diet so that you know how it works.
Gut-friendly behaviors and practices are part of the system as well as identifying and addressing underlying causes that are specific to your case of LPR.
For more information about the Fast Tract Diet, please read the Fast Tract Digestion Heartburn book which also applies to LPR.
For individual consultation, you can reach me through our contact form.
Final note
LPR is a subtle but persistent irritation that will take some time to heal after stopping reflux. To succeed, you must effectively stop reflux for several weeks to several months for full resolution of these symptoms.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment
You must be logged in to post a comment.