

Someone recently posted a question: “Don’t fats loosen the LES or lower esophageal sphincter causing reflux?”
For decades, dietary recommendations for GERD (gastroesophageal reflux disease) have focused on reducing fat intake. This is based on the 1973 study 1 suggesting that fats lower LES pressure and could lead to increased reflux episodes.
However, recent research challenges this view, highlighting fermentable carbohydrates as a more significant contributor to reflux.
🔍 Here’s what the evidence tells us
🍞 Carbohydrates and Reflux
Fermentation and Gas Production
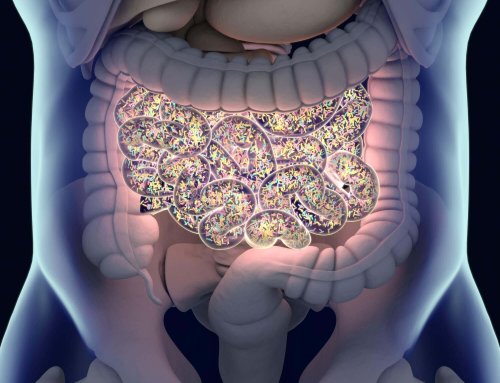
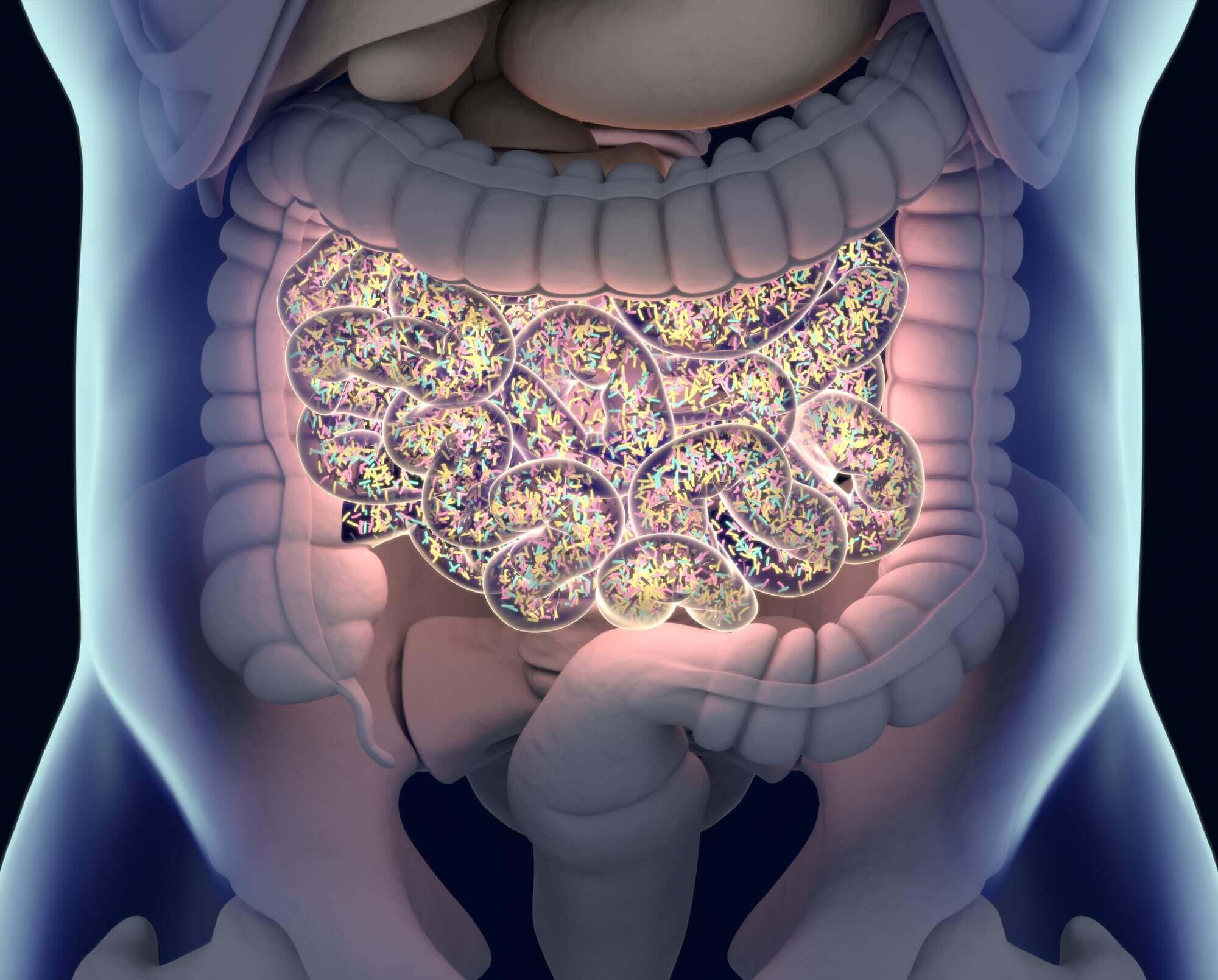
Bacteria in the gut ferment certain carbohydrates and produce gas. When you consume too many dietary carbs coupled with poor digestion, excessive gas builds up in your intestines. This leads to increased intragastric pressure in the stomach, which promotes reflux events. Previously, these events have been referred to as “transient LES relaxations.”
Intragastric pressure pushes the LES valve to open
When measured by a technique called manometry, it appears that the LES is “relaxing” during reflux. But this newer idea posits that intragastric gas pressure from fermentation is “pushing it to open,” like dropping a Mentos candy in a Coke bottle. I developed this theory and wrote about it in my books, Heartburn Cured and Fast Tract Digestion Heartburn.
🥩 Fats are NOT the problem
-
High-fat meals did not increase reflux when calorie content was controlled. Therefore, “it is inappropriate to advise GERD patients to reduce the fat content of their meals for symptom relief.” 2
-
The calorie content is more important than the fat content 3
-
Several more studies confirm that fats don’t cause reflux 4, 5
🍚 Carbohydrates are the problem
-
Studies show that dietary carbohydrate restriction is effective in relieving GERD symptoms and reducing esophageal acid exposure 6, 7
-
A more extensive study of 144 obese women with GERD resolved their GERD symptoms and stopped medication after 10 weeks on a high-fat, low-carb diet 8
💡 A Better Way to Manage Reflux
This research challenges the long-standing focus on fat reduction and supports a new dietary approach: limiting fermentable carbohydrates.
The Fast Tract Diet offers a science-backed solution that targets the real dietary triggers of reflux for both acid and non-acid reflux (LPR).
🦠 Not only that, the Fast Tract Diet addresses gut dysbiosis, including:
-
SIBO (hydrogen and/or hydrogen sulfide gas)
-
IMO (methane gas)
-
Other forms of dysbiosis (mixed gases and other end products)
This is because fermentable carbs, especially the five types targeted in the Fast Tract Diet, are the primary fuel source of gut microbes, thus potentially driving overgrowth and excessive gas production.
Overfed gut bacteria produce excessive amounts of gas.
Remember, 30 grams of unabsorbed carbohydrates allows bacteria to produce more than ten liters of hydrogen gas. 9
As a result, there have been well-documented explosions during intestinal surgery. 10, 11
🔬 Carbohydrates, gases, and the molecular food chain
-
Many (types of) bacteria ferment carbohydrates and produce hydrogen gas
-
Sulfate-reducing bacteria can convert hydrogen to hydrogen sulfide
-
Archaea can convert it to methane
Thus, carbohydrates are connected to different forms of dysbiosis.
🧭 Take the Next Step Toward Relief and Recovery
Step 1
📘 To address acid and non-acid reflux based on the latest science and gut dysbiosis, read theFast Tract Digestion Heartburn book.
Step 2
📱 Ready to implement the Fast Tract Diet? Use the Fast Tract Diet app.
Step 3
🗓️ To fully address your reflux and gut dysbiosis-related digestive and overall health issues, call us at (844) 495-1151 (US) from 8:30 a.m. to 5:00 p.m. ET, Monday through Friday.
But…
Now, you might ask:
“What do I do if I cannot tolerate fats?”
“I need carbs because I don’t want to lose weight.”
“I am on a plant-based diet, so I can’t do it.”
There are 35–40 common underlying causes for functional gastrointestinal disorders like reflux and different forms of gut dysbiosis. Customized strategies based on your dietary preference are available through consultation.
To fully address your reflux and/or gut dysbiosis-related digestive and overall health issues, call us at (844) 495-1151 (US) from 8:30 a.m. to 5:00 p.m. ET, Monday through Friday.
Identifying and addressing the underlying causes in your specific case must be part of the overall strategy.
📚 References
-
Nebel, O. T., & Castell, D. O. (1973). Inhibition of the lower oesophageal sphincter by fat—A mechanism for fatty food intolerance. Gut, 14(5), 270–274. PMC1412588
-
Pehl, C., Pfeiffer, A., Wendl, B., & Kaess, H. (1999). Effect of low and high fat meals on lower esophageal sphincter motility and gastroesophageal reflux in healthy subjects. The American Journal of Gastroenterology, 94(5), 1192–1196. PubMed: 10235191
-
Colombo, P., Mangano, M., Bianchi, P. A., & Penagini, R. (2002). Effect of calories and fat on postprandial gastro-oesophageal reflux. Scandinavian Journal of Gastroenterology, 37(1), 3–8. PubMed: 11843031
-
Penagini, R., Mangano, M., & Bianchi, P. (1998). Effect of increasing the fat content but not the energy load of a meal on gastro-oesophageal reflux and lower oesophageal sphincter motor function. Gut, 43(3), 330–334. PMC1727046
-
Ruhl, C. E., & Everhart, J. E. (1999). Overweight, but not high dietary fat intake, increases risk of gastroesophageal reflux disease hospitalization: the NHANES I Epidemiologic Followup Study. The American Journal of Gastroenterology, 94(5), 1192–1198. PubMed: 10501410
-
Yancy, W. S., Provenzale, D., & Westman, E. C. (2001). Improvements of gastroesophageal reflux disease after initiation of a low-carbohydrate diet: Five brief case reports. Alternative Therapies in Health and Medicine, 7(6), 120–123. ProQuest
-
Austin, G. L., Thiny, M. T., Westman, E. C., Yancy, W. S. Jr., & Shaheen, N. J. (2006). A very low-carbohydrate diet improves gastroesophageal reflux and its symptoms. Digestive Diseases and Sciences, 51(8), 1307–1312. PubMed: 16871438
-
Pointer, S. D., Rickstrew, J., Slaughter, J. C., Vaezi, M. F., & Silver, H. J. (2016). Dietary carbohydrate intake, insulin resistance and gastro-oesophageal reflux disease: a pilot study in European- and African-American obese women. Alimentary Pharmacology & Therapeutics, 44(3), 283–293. PubMed: 27582035
-
Suarez, F., & Levitt, M. (2001). Gas production from carbohydrates. In Bosker, G. (Ed.), Textbook of Primary and Acute Care Medicine (2nd ed., p. 1191). Print
-
Inan, A., Dener, C., & Demirci, S. (2003). Explosion during diathermy gastrotomy in a patient with carcinoma of the antrum. Surgical Endoscopy, 17(4), 651. PubMed: 14627190
-
Bigard, M. A., Gaucher, P., & Lassalle, C. (1975). Fatal colonic explosion during colonoscopic polypectomy. Endoscopy, 7(2), 105–106. PubMed: 499716




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment
You must be logged in to post a comment.